SEVERE STENOSIS LMCA (Similar findings with severe 3-vessel disease. This is a non-STEMI)
First let us address the case of acute total occlusion of the LMCA.
The vast majority of these patients will die before arrival to the hospital. Their death is due to injury to massive amounts of myocardium and electrical conduction tissue. Pump failure and electrical malfunction will usually result in death. Therefore we will instead address the case of acute onset of “severe stenosis” of the LMCA and ask the question:
What changes would I expect to find on the 12-Lead ECG with “severe stenosis” of the Left Main Coronary Artery?
DISCUSSION
The hemodynamic affect of severe stenosis of the Left Main Coronary Artery will result in subendocardial ischemia/infarction in the areas supplied by this artery. The ECG manifestations will be widespread ST Depressions plus T- wave inversions especially in Leads of the inferior, lateral, high-lateral area i.e. Leads I, II, avF, avL, V3,V4 V5, V6 (maximum depression in V4, V5, V6)
The vector representation of this ST event would be a dominance of vectors pointing in a leftward-downward direction. See Illustration 18 and notice I have labeled most of the arrow heads with STD to emphasize that the dominance of the energy wave is in a leftward-downward direction and furthermore is ST Depression.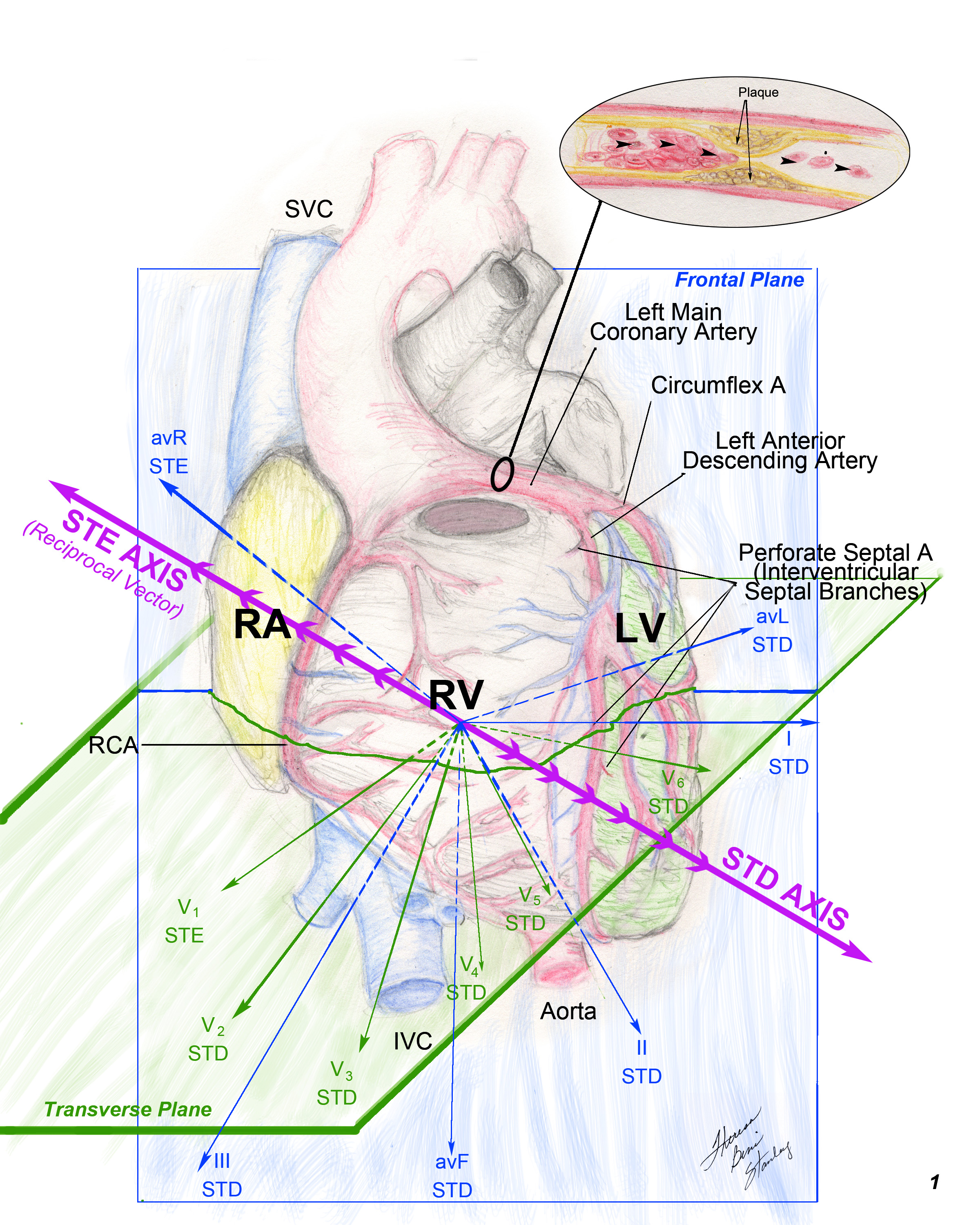
Illustration 18 LMCA Severe Stenosis Vector Diagram.
Let us now brain-storm this issue with a series of questions, statements and one-liners:
If most of the electrical wave (ST depressions) is in a leftward-downward direction…
For the sake of argument we will replace all those vectors with a resultant vector (similarly as we do with electrical axis)
For the sake of discussion we will call this ST Depression vector resultant ⇒ (DAxis⇒). It is a vector pointing in dominantly the V5,V6 direction and downward.
Mentally sketch in the reciprocal vector and give it the name ST Elevation vector resultant (EAxis⇒ )
It is of note that the EAxis⇒ is pointing in the general direction of Lead avR and Lead V1.
If the ST segment of vector DAxis⇒ is depressed, where will the ST segment of the vector EAxis⇒ lie ? →→
Answer – it will demonstrate ST Elevation.
How is this discussion useful in electrocardiography? This requires mental gymnastics.
Answer: Regarding the ST Segment…
You should routinely mentally sketch in the DAxis⇒
Then mentally sketch in the EAxis⇒
If the EAxis⇒ is pointing toward the right shoulder in a given cardiogram and widespread ST Depression is present and STE in Lead avR is present.→→→
You are most likely dealing with severe stenosis of the LMCA or severe multiple vessel disease. In the setting of ACS, either one of these diagnoses is life threatening and the patient might need to go for cardiac cath if you are unable to stabilize the patient or symptoms worsen. The treatment mode will depend on the clinical environment such as symptoms controlled, hemodynamic stability, exclusion of other differential diagnoses and comparison with old tracings.
ONE-LINERS re LMCA SEVERE STENOSIS (OR SEVERE MULTIPLE VESSEL DISEASE; this is a non-STEMI)
- Highly probable LMCA severe stenosis or severe multivessel disease if
- Widespread STD plus T-wave inversions in Leads I,II, avF, avL,V3V4,V5, V6 (maximum in V4, V5, V6; DAxis⇒ is pointing leftward-downward).
- STE in Lead avR ≥ 1 mm and NSTEMI, it most likely is a LMCA severe stenosis/3-VD and the patient will likely need CABG surgery.
This is a non-STEMI. Do not give thrombolytics.
- Try to avoid clopidogrel (Plavix) since many of these patients are likely to need urgent CABG surgery.
- Patients with acute total occlusion of LMCA usually die prehospital.
- STE in Lead avR is useful predictor of poor outcome and of need for CABG surgery.
- Absence of STE in Lead avR essentially excludes significant LMCA stenosis.
- If STE in Lead avR > STE Lead V1, this supports the diagnosis of severe stenosis LMCA/3-VD.
- Diagonal Artery supplies blood to lateral, high-lateral area of heart.
- Both severe multivessel disease and severe stenosis LMCA might need urgent CABG surgery.
- Be sure you have considered other differential diagnoses such as
DIFFERENTIAL DIAGNOSES OF SIMILAR ECG PATTERNS (partial list; these disorders can present with similar ECG changes)
- Pulmonary embolus.
- Hypoxemia
- Tachycardia
- Severe hypertension
- Anemia
- Acute pulmonary edema
- COPD exacerbation
- Hypotension
- Sepsis
In summary, you would need to address the underlying pathology, then reassess the patient including a repeat ECG. You might find that following correction of the disorder eg tachycardia, the symptoms as well as ECG abnormalities resolve. The symptoms and ECG might not represent coronary artery stenosis at all!
PEARL
1. Please be aware that acute severe stenosis of LMCA is just a step away from total occlusion and high risk of death. Therefore, although it is not a STEMI, it is a dangerous situation and sometimes the patient needs to go to the cath lab urgently, sometimes because of hemodynamic instability and worsening pain in spite of treatment. As always, clinical correlation applies.
2. General guideline
a. If it is a NSTEMI and you find STE in Lead avR ≥ 1 mm →→ consider holding plavix. Discuss with cardiologist or cardiovascular surgeon since patient may need CABG surgery.
b. If it is an NSTEMI and you find STE in Lead avR < 1 mm →→ unlikely to need CABG surgery, therefore it might be ok to give plavix.
IN CONCLUSION:
Regarding the analysis of the 12-Lead ECG ACS patient it is important to consult with Lead avR. Specifically we are looking for STE in Lead avR to aid us with the differential diagnoses including:
- LMCA severe stenosis / 3- VD (NSTEMI)
- LAD (proximal) total occlusion STEMI)
This decision will direct your treatment plan such as:
- Medication including ± clopidogrel (Plavix)?
- Thrombolytics?
- To cath lab urgently?
- Realization that the patient might be a candidate for CABG surgery?
- Need to discuss findings with the Cardiologist / cardiovascular surgeon, as you proceed with stabilization treatment in the emergency unit?
Key to Abbreviations:
STD … ST Depression
STE … ST Elevation
LAD … Left Anterior Descending Coronary Artery
LMCA … Left Main Coronary Artery
LCx … Left Circumflex Coronary Artery
RCA … Right Coronary Artery
LV … Left Ventricle
RV … Right Ventricle
LBBB … Left Bundle Branch Block
RBBB … Right Bundle Branch Block
STEMI … Acute total occlusion of a coronary artery
NSTEMI … Myocardial infarction without total occlusion of a coronary artery
ACS … Acute Coronary Syndrome
3-VD … Multi-vessel coronary artery disease
RBB…Right bundle branch
LBB…Left bundle branch
Now please click on the link below to start Quiz 3 in order to progress to Module 4.