(C) 2025 ECGcourse.com LLC. All Rights Reserved | Author: Vernon R Stanley, MD, PhD | Editor: Courtney Stanley, MS, PA-C
Why ECG changes from LVH are crucial to your patient’s cardiac care
A patient’s ECG shows changes from LVH (Left Ventricular Hypertrophy). But why is it important to learn how LVH can alter the ECG?
In this post, we will discuss three things you need to know about LVH. Please know that these are by no means the only three things you need to know about LVH. But it is important to know that LVH is a notorious boobytrap of electrocardiography interpretation; therefore, it can present a great challenge to the interpreter. So, for the brevity of this post, we will refine the discussion to three points. For a deeper discussion and understanding of LVH, we encourage you to read more about our comprehensive, Advanced 12-lead ECG Course (30 hours Cat I CME/CE).
Blog Objectives:
- Learn the diagnostic criteria of LVH (Left Ventricular Hypertrophy)
- Look for “pseudo-infarction” patterns sometimes seen secondary to LVH
- Be aware of “pseudo-LVH” which may occur in the presence of LBBB, LAFB or WPW
ECG Challenge Quiz
*Answers at bottom of post.
- True/False: The criteria for LVH on ECG is very sensitive, but it is not very specific.
- LVH may cause the following patterns on the 12-lead:
- Significant Q-waves (> 0.04 sec | 1mm wide)
- Irregular Ventricular Rhythm (QRS-QRS interval)
- Short PR interval < 0.12sec
1. LVH (Left Ventricular Hypertrophy) Criteria
First, let’s review some general guidelines and criteria to help you recognize LVH (Left Ventricular Hypertrophy) on the 12-lead ECG. Please know these are general guidelines and not black and white, hard rules. As always, clinical correlation with patient presentation, lab results, serial ECGs and comparison with an old ECG as well as consult with the cardiologist or attending physician are always recommended.
The term hypertrophy, according to Dorland’s Online is generally defined as “an increase in the volume of a tissue or organ produced entirely by an enlargement of existing cells.” Regarding LVH, we are specifically referencing enlargement or hypertrophy of the Left Ventricle, often secondary to prolonged hypertension or valvular disease.
Enlargement of the Left Ventricle is significant in terms of the because of the voltage contribution from the left ventricle which is seen in the leads which “look” at the left ventricle: Leads V1-V6 (the precordial leads) and also Lead I and avL (the lateral and high lateral leads). Below is a diagram which shows the depolarization of the wavefront through the myocardium and then produces the resultant waveform captured by the electrode, either moving toward the electrode or away from the electrode.
For general criteria of LVH (Left Ventricular Hypertrophy), we will agree to the following:
*As a rule of thumb, we will use > 35 years of age as a cutoff to LVH. Some sources adjust this age to 40; but for our discussion’s sake, we will agree to > 35 years.
*The criteria for LVH are specific; the criteria are not very sensitive. In other words, If LVH is present on the ECG, the patient has the condition (specificity). To the contrary, may people who have LVH, do not have ECG which reveal it (sensitivity).
*(1) The Tallest S of V1 V2 V3 + The Deepest R of V4 V5 V6 > 35mm
OR
(2) R voltage of Lead avL > 12mm
OR
(3) R-wave voltage or S-wave voltage > 20mm in any Limb Lead (I, II, III, avR, avL, avF)
OR
(4) R-wave voltage or S-wave voltage > 25mm in any precordial lead (V1-V6)
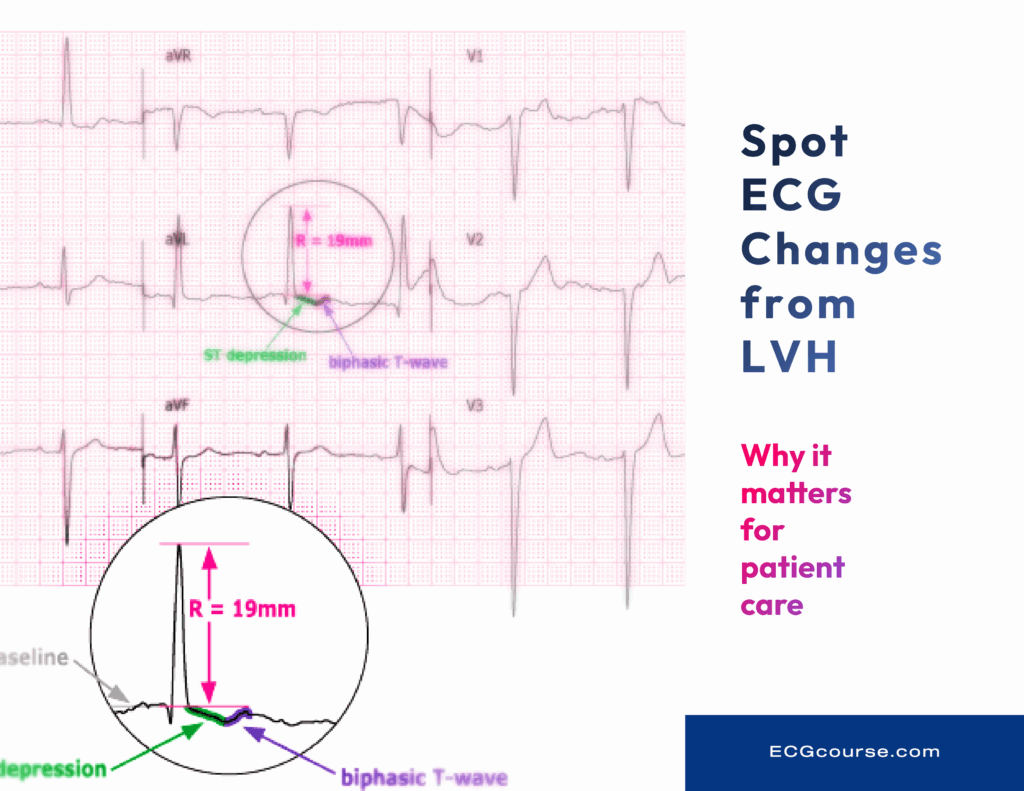
2. LVH is one of the great “boobytraps” of electrocardiography. Here are 3 “Pseudo-infarction” Patterns seen on ECG which are changes secondary to LVH (Example 12-lead ECG)
The LVH is known to distort the 12-lead ECG and often causes dramatic changes in the waveform. Therefore, it is important to recognize LVH as one of the great boobytraps of ECG interpretation. (LBBB is the other boobytrap, which we have also discussed in detail – Finding a STEMI in the presence of the Left Bundle Branch Block (LBBB) ECGcourse.com).
These dramatic waveform changes may be seen in many of the leads of a 12-lead ECG. However, these ECG changes are sometimes only present in one lead of the full 12-lead. These changes are often referenced clinically as “LVH with Strain”.
- ST Elevation or Depression
- T-wave Peaking and/or Inversion
- Significant Q-waves (often in Leads V1 V2 V3)
The following 12-lead ECG tracing is from an 82-year-old patient. It highlights these striking changes which appear eerily similar to an acute Anterior MI (STEMI).
Sample 12-lead ECG of “LVH with Strain”
This classic example of “LVH with Strain” highlights why comparison with an old ECG when available is critically important as well as clinical correlation and serial ECG and enzyme monitoring.
For further discussion on the LVH pattern and changes which it can cause to the 12-lead, please see the Advanced 12-lead ECG Course.
3. Pseudo-LVH in Presence of LBBB, LAFB or WPW
Important Clinical Pearl
In the presence of LBBB, LAFB or WPW, the general criteria of LVH as listed above may not be valid. In these cases, the appropriate designation would be “pseudo-LVH”. “Pseudo-LVH” may also be present in the very young who exhibit high voltages, as well as endurance athletes (i.e. professional cyclists).
We will discuss this further in an upcoming blog. But for now, we will agree that in the presence of LBBB, LAFB or WPW, the general criteria of LVH may not be valid.
*ECG Changes from LVH Answer Key
- True/False: The criteria for LVH on ECG is very sensitive, but it is not very specific.
- LVH may cause the following patterns on the 12-lead:
- Significant Q-waves (> 0.04 sec | 1mm wide)
- Irregular Ventricular Rhythm (QRS-QRS interval)
- Short PR interval < 0.12sec
Additional Reading on LVH
- LVH (Left Ventricular Hypertrophy) as a STEMI Mimic ECGcourse.com
- Left Ventricular Hypertrophy (LVH) • LITFL • ECG Library Diagnosis
- ECG in left ventricular hypertrophy (LVH): criteria and implications – The Cardiovascular
- Left Ventricular Hypertrophy in the Electrocardiogram
- JMS-007-DEBASIS-Pseudo-LVH.pdf
Questions about this Blog, a new or previous order? Contact Us.
Recommended products
-

50 ECG Case Studies Course (13 Hrs CME)
$145.00 -

Advanced 12-Lead ECG Interpretation Course (30 Hrs CME)
$499.00 -
50 ECG Case Study & STEMI Review Combo Pack (19 Hrs CME)
Original price was: $235.00.$199.00Current price is: $199.00. -
HEART Ruler Mnemonic Pocket Guide
Original price was: $15.00.$9.95Current price is: $9.95. -
12-lead Textbook, Workbook & HEART Ruler Packet
Original price was: $124.00.$110.00Current price is: $110.00. -
Intensive Triple Bundle ECG Course Suite: (52 Hrs Cat I CME/CE)
Original price was: $769.00.$699.00Current price is: $699.00. -

12-lead ECG Interpretation Workbook
$48.50 -
BOGO: 12-lead ECG Course + 50 ECG Case Study Course (43 Hours Cat I CME/CE) | 50% Off
Original price was: $644.00.$569.00Current price is: $569.00.
")



