V.R. Stanley, MD, PhD © 2018. All rights reserved.
As Medical Director for an emergency group, you have been asked to interpret the tracing below of a 60 year old female with chest pain.
INTERPRETATION:
Acute ST-elevation MI (Inferior) (STEMI)
DISCUSSION:
Let us analyze the tracing using the acronym H-E-A-R-T. We will then take these findings and place them in clinical perspective.
“HEART” ACRONYM ANALYSIS
H…………Hypertrophy
No evidence of LVH
No evidence of RAE
No evidence of LAE
E………. Extent of intervals
PR interval……………….Normal
QRS duration……………Normal
QT interval……………….Normal
A………………Axis
Lead I and Lead aVF are both positive. The axis is therefore Normal.
R………………qRs-st analysis
Small Q-waves noted in Leads II, III, aVF (insignificant width)
Normal R-wave progression
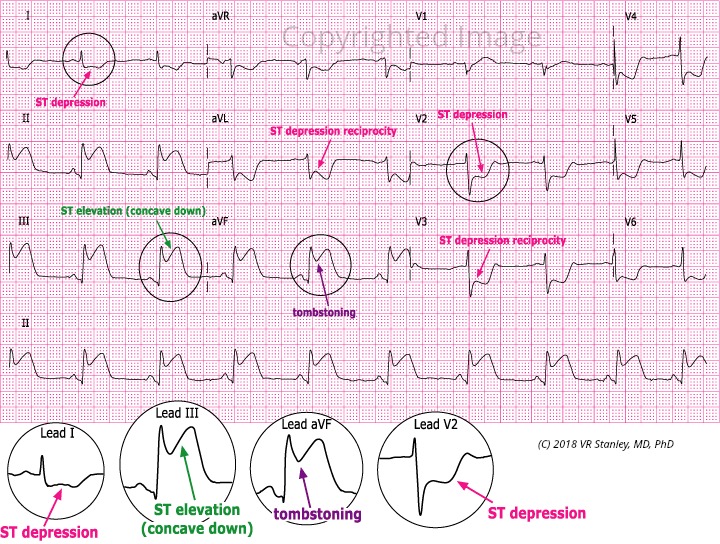
ST elevation (concave down) in Leads II, III, aVF
ST-depression in Leads I, aVL, V2 thru V6
T………….T-waves
T-wave peaking in Leads II, III, aVF
T-wave inversion or biphasic T’s in Leads I, aVL, V2 thru V6
SUMMARY OF SIGNIFICANT FINDINGS
1. ST-elevation (concave down) Leads II, III, aVF
2. ST-depression Leads I, aVL, V2 thru V6
3. T-wave inversion (or biphasic T’s) Leads I, aVL, V2 thru V6
LESSON NOTE ON THE ACUTE ST-ELEVATION MI
As we search to recognize the pattern of the Acute ST-elevation MI, I want to warn you of the two greatest booby traps of electrocardiography: the LBBB pattern and the LVH pattern. Both these patterns frequently modify the cardiogram and their characteristics frequently ” look like ” the acute MI and/ or an old MI patterns, but alas they are pseudopatterns.
In summary the LVH and the LBBB frequently exhibit the following characteristics:
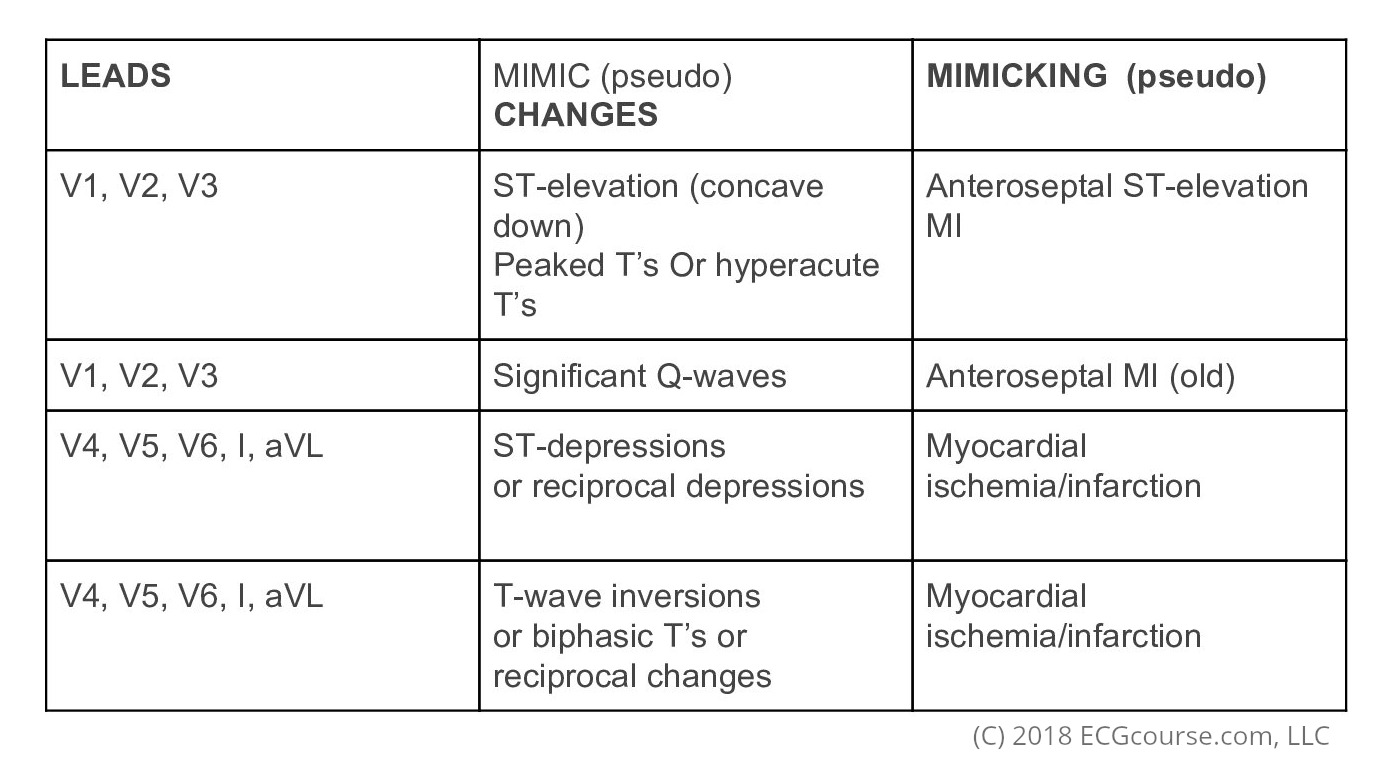
REMEMBER: The changes described above are actually NOT usually ischemia/infarction but are pseudopatterns and simply a part-and-parcel of the LBBB and LVH pattern.
You will notice the absence of the LBBB and LVH in this Case Study tracing. When this is the case, we can make the following general conclusion:
RULE: If you find ST-segment elevation (concave down) in the associated leads and ST depression/T-wave inversion in the reciprocal leads, this is virtually diagnostic of the Acute ST-Elevation MI (STEMI).
.
In this Case Study tracing I have circled, magnified, color-code labeled Leads I, III, avF, V2.
It is clearly true that this tracing satisfies the RULE as given above with the following agreed Associated-Reciprocal guideline.
AREA OF HEART……………..ASSOCIATED LEADS………………….RECIPROCAL LEADS
Inferior ( Diaphragmatic )………………..II, III, aVF…………………………………….I, aVL, V1 thru V6
Septal……………………………………………..V1, V2………………………………….V3 thru V6, I, aVL, II, III, aVF
Anterior……………………………………….V2, V3, V4………………………………..V5, V6, I, aVL, II, III, aVF
Lateral………………………………………….V4, V5, V6………………………………V1, V2, V3, I ,aVL, II, III, aVF
High Lateral……………………………………..I, aVL……………………………………….all other leads
Right Ventricle…………………………………V4R * ……………………………………….V4, V5, V6, I , aVL, II, III, aVF
Posterior…………………………………………V8, V9 * ……………………………………V1 thru V6, I, aVL
* See page Appendix A18-24 of Dr. Stanley’s Textbook
SUMMARY INTERPRETATION
We find ST-Elevation (concave down) in the inferior associated leads of II, III, aVF with ST-depression and T-wave inversion in the reciprocal leads of I, aVL, V2 thru V6. This is virtually diagnostic of the Acute Inferior MI (STEMI).
INTERPRETATION:
Acute ST-elevation MI (Inferior; STEMI)
The treatment response would depend on your environment and availability of cardiology back-up but would include either
- Aggressive medical treatment including thrombolytics, then transfer to a cardiac center.
OR
2. Pre-medicate and transfer directly to the cardiac cath lab.
One Response