(C) August 30th, 2023 Vernon R Stanley, MD, PhD | Courtney Stanley, PA-C Editor | ECGcourse.com LLC All rights Reserved.
Please answer the following pre-blog questions. Answers at bottom of post.
Q1. In the case of Acute Pericarditis, 12-lead ECG changes may include:
- ST elevation in leads II, III & avF
- ST elevation diffuse in nearly all leads
- |QRS| > 0.20 sec
- Ventricular Quadrigeminy
Q2. Benign Early Repolarization (BER) is a common, normal 12-lead ECG variant. It is most likely present if which of the following exists:
- A. The presence of J-point elevation
- B. ST segment elevation present in most of the leads
- C. ST-segment elevation concave up (holds water)
- D. Only can be present if the patient is younger than 18 years old
- E. None of the above
- F. A, B & C only
Q3. On the 12-lead ECG, pericarditis is a more likely diagnosis than Acute STEMI if:
- A. ST segment changes are present in associated and reciprocal leads
- B. Wide, new Q-waves are present in associated leads
- C. The patient experiences some pain relief when sitting up
- D. The patient has a fever
- E. All of the above
- F. C & D only
What is Pericarditis?
Pericarditis is an inflammation of the fibrous sac around the heart, the pericardium. Approximately 30% of patients who experience an episode of acute pericarditis will have more than one episode.
Clinical symptoms of Pericarditis:
-
- Mid-pleuritic chest pain
-
- Pain worsens with recumbency
-
- Fever (+/-)
-
- Pain relieved by leaning forward
-
- Pericardial friction rub may be present
Causes of pericarditis include but are not limited to:
-
- Infection: may be bacterial, fungal or viral, including HIV
-
- Acute Myocardial Infarction
-
- Immune-related: SLE (Systemic Lupus), rheumatoid disease
-
- Drug related: seizure meds, anti-coagulants
-
- Open heart surgery
-
- Radiation
-
- Uremia
-
- Malignancies
-
- Post Myocardial Infarction
-
- COVID
-
- Tuberculosis
ECG changes seen in Pericarditis
-
- Diffuse ST-segment elevation concave up (except Leads avR, V1)
-
- ST-segment depression Leads avR, V1
-
- Diffuse PR-segment depression (except Leads avR, V1)
-
- May exhibit PR-segment elevation in ECG Leads avR, V1
-
- May mimic Acute STEMI (ST Elevation Myocardial Infarction) or Benign Normal Variant (Benign Early Repolarization, aka BER)
-
- Lack of reciprocal ST-segment changes
-
- R-wave progression on ECG usually normal
-
- Quotient ST/T = mm of ST segment elevation / mm height of T-wave > 0.25 mm in Lead V6
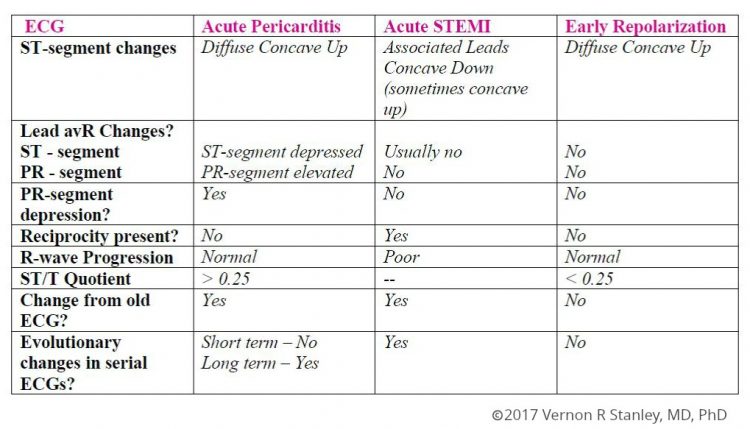
How to distinguish Acute Pericarditis vs STEMI vs Benign Repolarization
Distinguishing between acute pericarditis on ECG versus acute ST elevation MI (STEMI) and benign early repolarization (BER) can be a daunting task. We have created this quick-reference chart to compare pericarditis with STEMI and early repolarization. However, it is always most important to correlate with the patient’s clinical presentation, an old ECG when available, labs, chest film, serial ECGs and cardiac markers as well as consult with the referring physician, PCP and cardiology.
Examples of Acute Pericarditis on ECG | Tracing A & B
Here we will compare two 12-lead ECG tracings from the same patient. Tracing A is the current ECG. 12-lead Tracing B is from the same patient, 1 year prior.
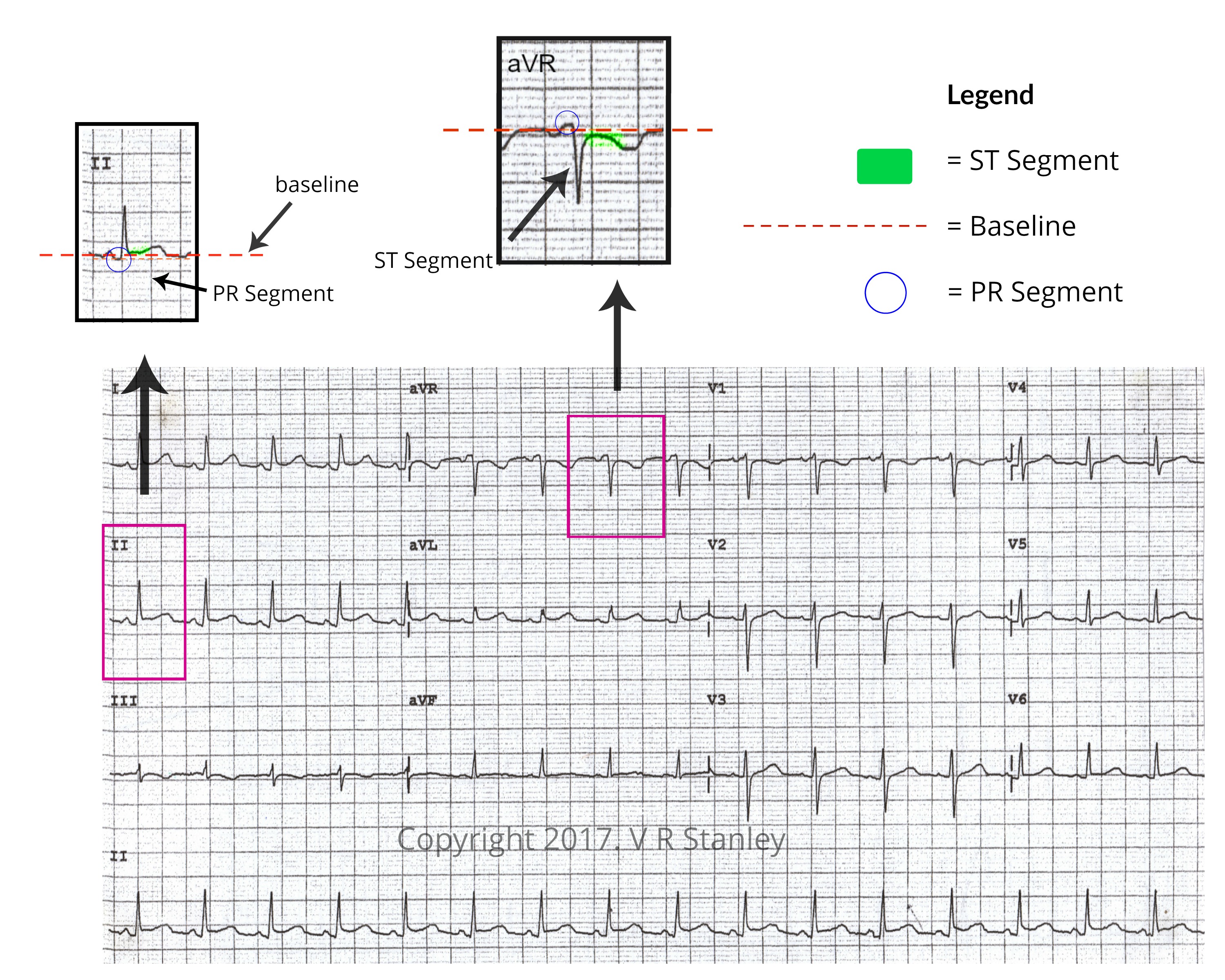
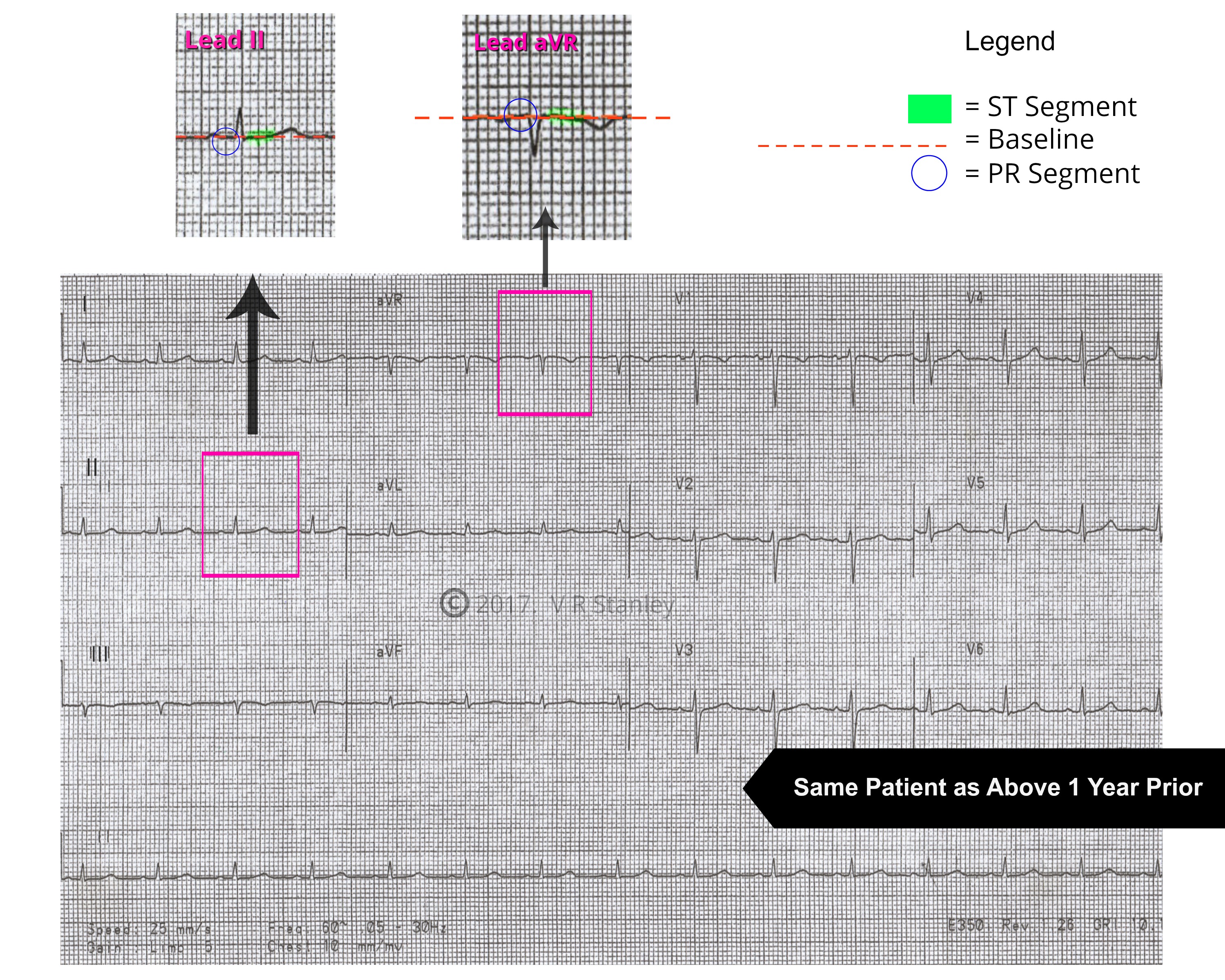
After review of the two 12-lead ECG tracings above, the current ECG demonstrates an ST segment that is elevated and a PR segment that is depressed (below the baseline). By comparison with the previous ECG from 1 year prior, the ST segment and PR segment are both at baseline, supporting that this patient does have acute pericarditis on ECG findings during current presentation (ECG Tracing A).
Benign Normal Variant (BER) on ECG
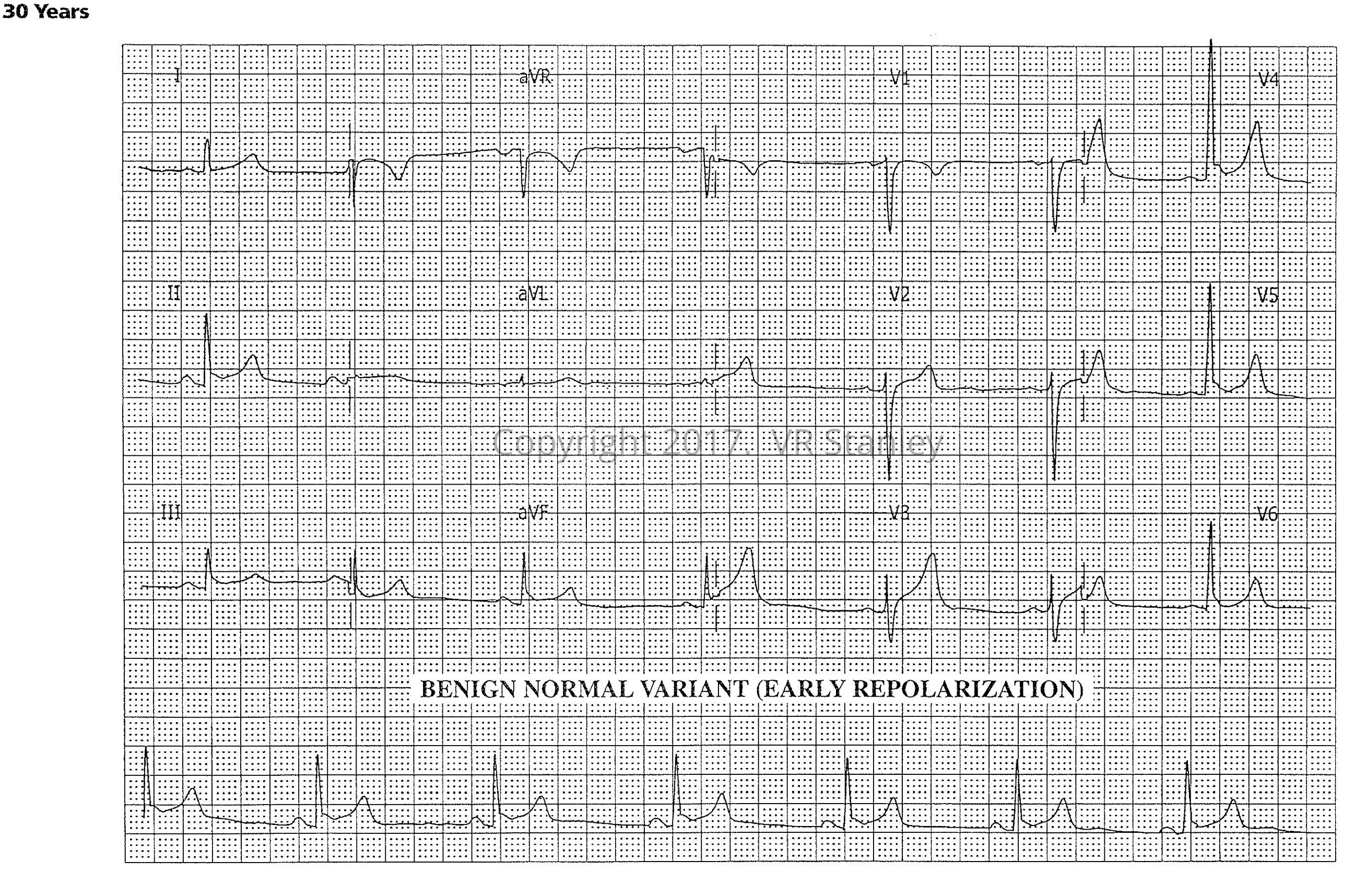
Benign Normal Variant (Early Repolarization)
During your daily practice of medicine, you are frequently faced with the following scenario:
You are presented with a cardiogram which demonstrates minor, subtle ST-segment elevations concave up. After analyzing the tracing, you have narrowed your choices to:
- Benign Normal Variant (Early Repolarization).
- Early, suspected Acute STEMI.
The sobering ramifications of this decision-making are obvious. On the surface, this challenge might appear to be straightforward; but in the clinical world you will encounter tracings that challenge even the most expert eye.
General comments regarding Early Repolarization Pattern
- Serial tracings will show essentially no changes evolving (unless an infarction is evolving also)
- Early Repolarization patterns essentially never show “terminal QRS distortion” (further discussion in our post on Terminal QRS Distortion)
For more information STEMI and STEMI patterns, we reference you to some of our previous, detailed posts:
- Acute Inferior STEMI – ECGcourse.com
- Posterior MI – the Hidden STEMI – ECGcourse.com
- Finding a STEMI in the presence of the Left Bundle Branch Block (LBBB) – ECGcourse.com
- WPW: “The Great Imposter” | STEMI Mimic – ECGcourse.com
Pre-quiz Answer Recap
Q1. In the case of Acute Pericarditis, 12-lead ECG changes may include:
- ST elevation in leads II, III & avF
- ST elevation diffuse in nearly all leads
- |QRS| > 0.20 sec
- Ventricular Quadrigeminy
Q2. Benign Early Repolarization (BER) is a common, normal 12-lead ECG variant. It is most likely present if which of the following exists:
- A. The presence of J-point elevation
- B. ST segment elevation present in most of the leads
- C. ST-segment elevation concave up (holds water)
- D. Only can be present if the patient is younger than 18 years old
- E. None of the above
- F. A, B & C only
Q3. On the 12-lead ECG, pericarditis is a more likely diagnosis than Acute STEMI if:
- A. ST segment changes are present in associated and reciprocal leads
- B. Wide, new Q-waves are present in associated leads
- C. The patient experiences some pain relief when sitting up
- D. The patient has a fever
- E. All of the above
- F. C & D only
Additional suggested reading and resources
-
12-lead ECG Interpretation Textbook
$64.99 -
12-lead ECG Interpretation Workbook
$48.50 -
12-lead Textbook, Workbook & HEART Ruler Packet
Original price was: $124.00.$110.00Current price is: $110.00. -

50 ECG Case Studies Course (13 Hrs CME)
$145.00 -
50 ECG Case Study & STEMI Review Combo Pack (19 Hrs CME)
Original price was: $235.00.$199.00Current price is: $199.00. -
50 ECG Case Study Value Packet | Textbook, Workbook, HEART Ruler + 13 Hours Cat I CME
$273.49

One Response