Quick Quiz
Q1: The Mobitz II ECG Rhythm is distinguished by a ____________ PR interval when the P-wave is conducted.
Q2: The Mobitz I ECG Rhythm is distinguished by a _____________ PR interval until a P-wave is dropped.
Q3: True or False: In the presence of a 2nd Degree AV Block 2:1 rhythm, it is possible to definitively diagnosis Mobitz I versus Mobitz II.
(See answers at end of post.)
OVERVIEW: 2° AV BLOCK 2:1 —— Is this Mobitz I OR Mobitz II ?
We have previously outlined the diagnostic criteria of the Mobitz I and Mobitz II ECG rhythms and determined that the key to the diagnosis is the ratio of Ps:QRSs. Specifically, these ratio arrays are demonstrated in Figure 1 below.
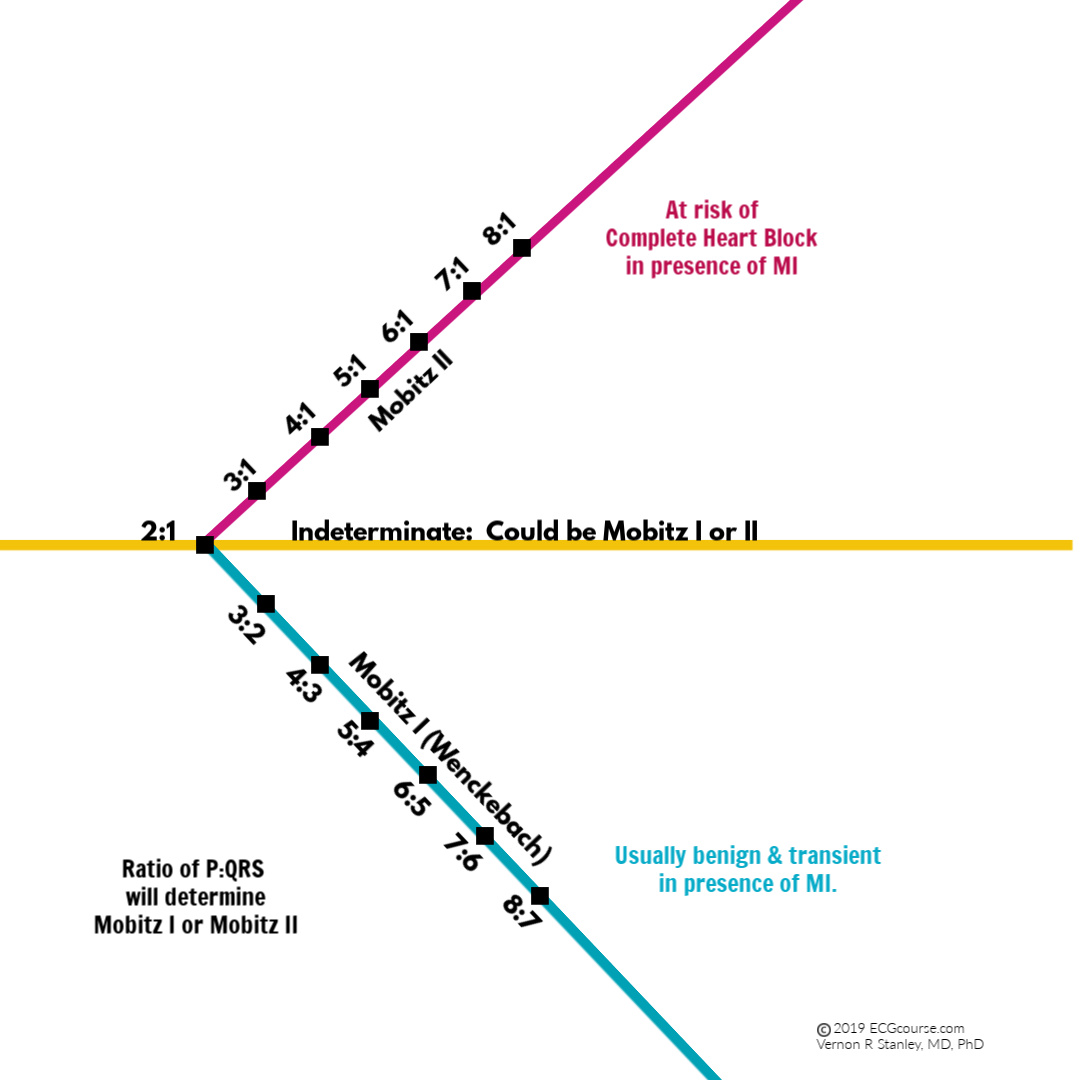
Figure 1 Ratios of P waves to QRS complexes
From Figure 1, it is interesting to note that the special case of P:QRS = 2:1 is an indeterminate one and the diagnosis could go either way (either Mobitz I or Mobitz II). You cannot be certain of the diagnosis, but you can at least suggest the probability of the diagnosis. This special case will be the focus of this lesson focusing on ECG Rhythms Mobitz I versus Mobitz II.
GOAL:
This lesson will discuss in detail the special case of the 2° AV block with a ratio of 2:1 block. We will concede that this is an indeterminate case but will conclude with a list of findings suggestive of Mobitz I or Mobitz II.
DISCUSSION
Second-degree AV block is rarely symptomatic and by itself is not dangerous. The question is whether second-degree block indicates increased risk for complete AV block and if so whether asystole is likely to occur.
AV node block (localized to the AV node-junction area) rarely progresses to third-degree block and often has a reliable escape rhythm if it does. If the block is localized to the HP (HIS bundle-Purkinje) level it is more likely to progress to complete block and is more likely to result in asystole. AV junction-node suppression typically results in Mobitz 1 Block, whereas HP block leads to Mobitz II block. Therefore, the Mobitz 2 Block places the patient at high risk for complete heart block and sudden death. In the presence of 2:1 AV block Mobitz 1 and 2 cannot be distinguished; a widened QRS complex and normal PR interval suggest that the AV block is at the HP (HIS Bundle – Purkinje) level.
PEARL: Atropine improves AV node conduction. It has no direct effect on HP (HIS Bundle-Purkinje) conduction but by causing increased sinus rate can paradoxically increase HP block and therefore should be avoided.
Regarding the special case of 2° AV Block with 2:1 conduction, please be aware of the following clinical pearls:
- In the setting of the acute Inferior MI→→→→→ the 2° AV block 2:1 conduction is likely to be Mobitz 1 (this most often is a benign self-limiting development and usually requires no treatment).
- In the setting of the acute Anterior MI→→→→→ the 2° AV block 2:1 conduction is likely to be Mobitz 2 (this is a life-threatening development and places the patient at risk for complete heart block. You should therefore be prepared for transthoracic cardiac pacing).
- If the PR-interval normal (≤ 0.20 sec) →→→→ the 2° AV block 2:1 conduction is likely Mobitz 2.
- If | QRS | > 0.10 sec (i.e. is widened) →→→→→ the 2° AV block 2:1 conduction is highly probable Mobitz 2.
- If Mobitz 1 →→→ Atropine will increase sinus rate. The conduction defect might improve and actually resolve.
- If Mobitz 2 →→→ Atropine might worsen the block and precipitate complete heart block. It is therefore a relative contraindication to administer Atropine in the presence of 2° AV block Mobitz 2.
- In the setting of the acute Anterior MI and 2° AV block 2:1 conduction →→→→ the development of a new LAFB is suggestive of Mobitz 2. We will revisit this topic in a future post.
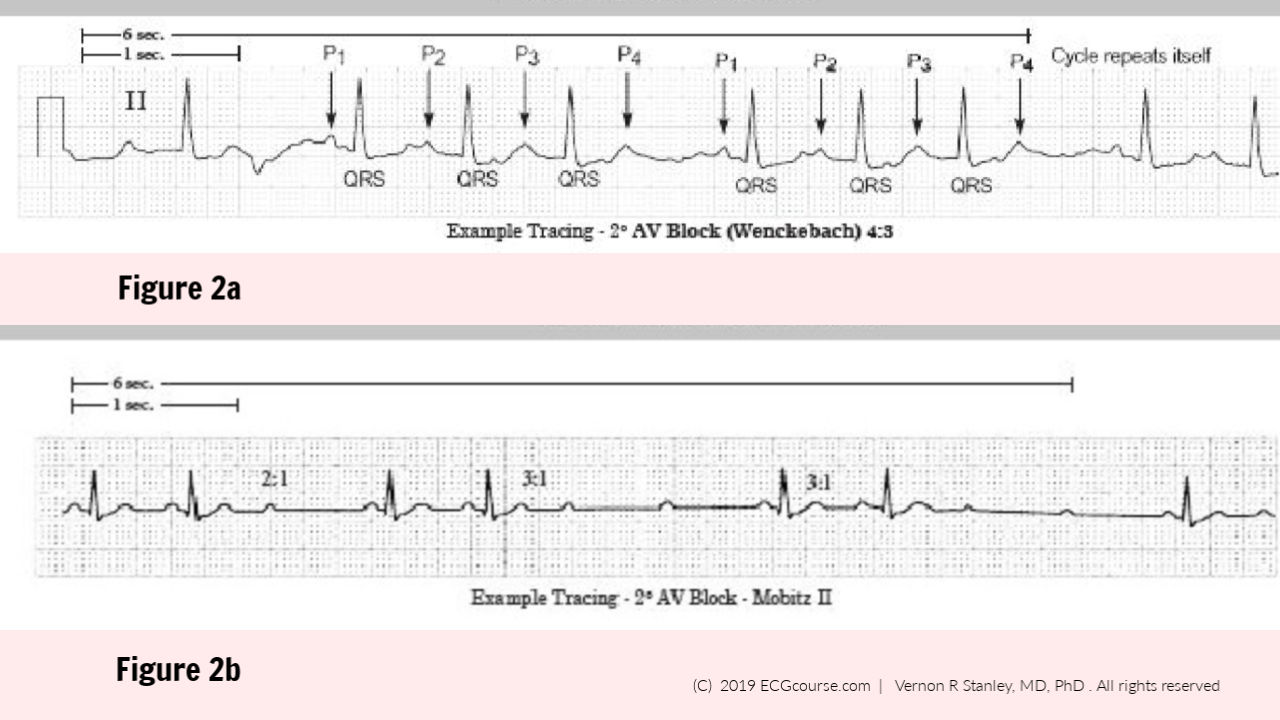
Let us begin this presentation by reviewing the characteristic of the two different 2° AV blocks – Mobitz 1 and Mobitz 2. First let me remind you of the characteristic rhythm pattern of the P-waves. This is best illustrated in the form of a rhythm strip as shown in Figure 2 (a & b)
When analyzing a given rhythm strip, I advise you to do the following:
- Photocopy the original tracing and use this as your working copy. You will feel free to mark, label, fold, erase, experiment with this copy since it does not become a part of the permanent record.
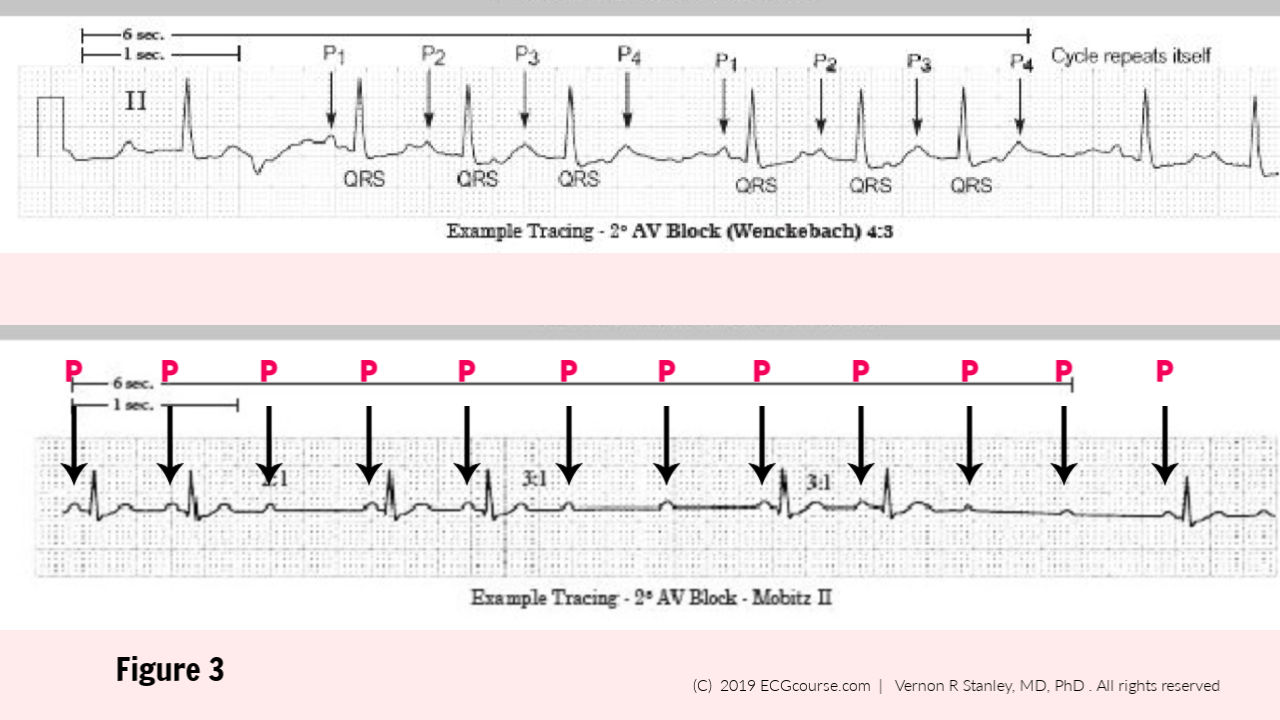
- With this copy, I recommend that you identify all the P-waves as shown in Figure 3.
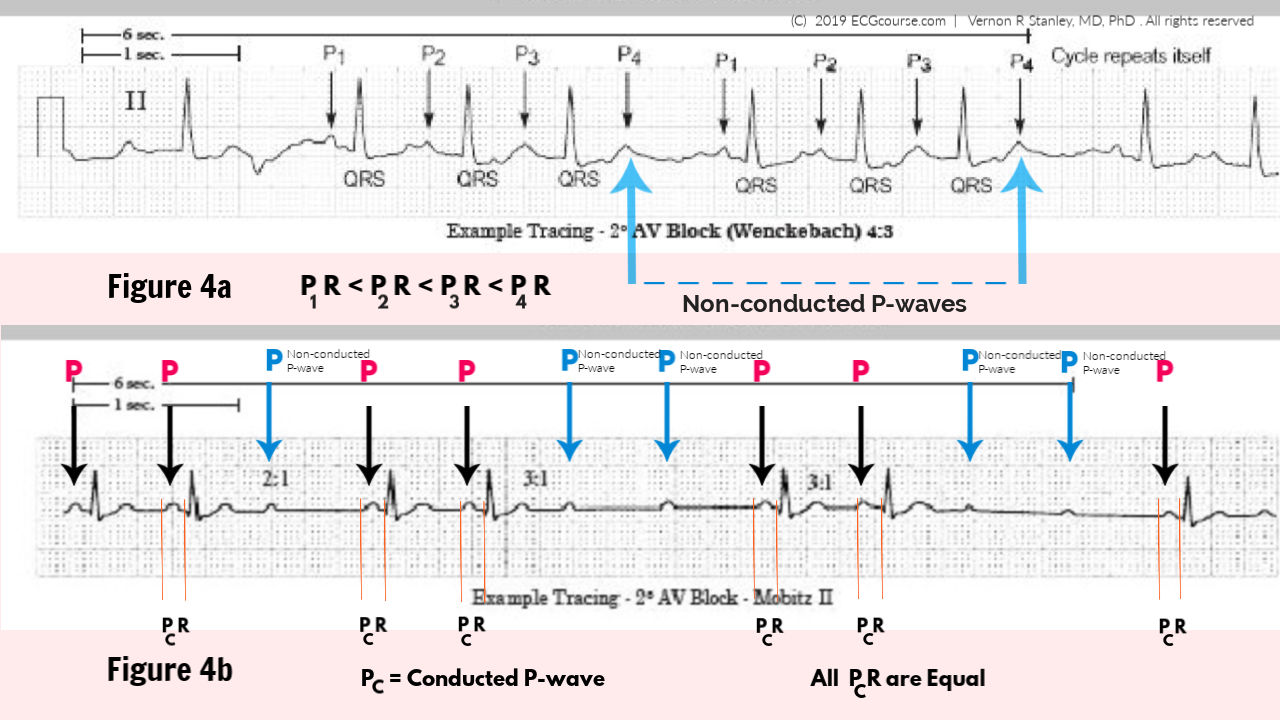
Now measure all the PR-intervals and determine their relationships with the P-Waves (if there is one), as shown in Figure 4 below.
Now let us consider the special case of 2° AV Block 2:1 (Mobitz 1 OR Mobitz 2). This is depicted in Figure 5 below. We observe the cyclic pattern of two P-waves for every one QRS complex. It is interesting to note that if the rhythm were Mobitz 1 (Wenckebach) you would need at least a P:QRS = 3:2 conduction in order to appreciate the progressive PR-interval phenomena. But alas, the ratio of Figure 5 is observed to be only 2:1. We must conclude that the interpretation of Mobitz 1 vs Mobitz 2 is indeterminate. In the clinical environment, I ask for a long rhythm strip hoping to find an area of 3:2 or 3:1 conduction indicating a diagnosis of Mobitz 1 or Mobitz 2 respectively. If this is not discovered, you can make the following likelihood of Mobitz 1 vs Mobitz 2:
a…..if PR-Interval > 0.20 sec→→→→→→ likely Mobitz 1.
b…..if |QRS| > 0.10 sec →→→→→→→→ likely Mobitz 2.
Now let us consider the rhythm strip below:

Figure 5 2° AV Block 2 : 1 |
It is clearly true that the ratio of P-wave to QRS complex is 2 to 1. This places this rhythm strip in the indeterminate category and the best you can do is to suggest the probability of either Mobitz 1 or Mobitz 2.
CLINICAL PEARLS:
- If you are unsure of the ECG Rhythm diagnosis, then ask for a 2-minute rhythm strip. This is approximately a 6-foot strip.
- Unroll the strip and lay it on the countertop.
- Inspect the full length of the strip with a magnifying glass (after all this IS a “Pink Panther” job) looking for a pattern OR lack of.
- Don’t forget to choose the lead that shows the P-wave most clearly. You should get in the habit of looking at ALL 12-leads, Right precordial and posterior leads.
- With both Mobitz 1 and Mobitz 2, the P-waves will march through at a regular cadence (please note there may be very slight variability in the P-wave cadence).
- You will be surprised at the enhanced insight achieved by choosing the lead which best shows the P and QRS complexes and printing off a long strip from this lead’s “viewpoint”.
CONCLUSION
When your analysis of a given rhythm strip reveals 2° AV Block with 2:1 conduction you must then concede that the further categorization of Mobitz 1 vs Mobitz 2 is indeterminate. The next step would be to analyze a long rhythm strip with the goal to discover a P to QRS ratio of 3:2, 3:1, 4:3. – thus making the diagnosis of either Mobitz 1 or 2.
If not found, you are limited to the following conclusion:
- a. If the PR-interval > 0.20 sec. →→→→→ probable Mobitz 1
- b. If the |QRS| > 0.10 sec. →→→→→ probable Mobitz 2 (highly probable)
- c. In the setting of the Acute Inferior MI →→→→→ probable Mobitz 1
- d. In the setting of the Acute Anterior MI →→→→→ probable Mobitz 2 (and is at risk for complete heart block)
Answers: Q1: constant | Q2: progressively lengthening | Q3: False
Article: ECGcourse.com | Vernon R Stanley, MD, PhD © 2024 All rights reserved.
Questions? Contact Us | To Compare all ECG and Rhythms Courses: Click Here.
7 Responses
I thought there would be verbal explanations of the rhythms. I would have preferred it to be so.
Hello! Thank you for your query. We do offer video and supplemental audio clips throughout the course. It may be found on each tutorial page of the Animated Rhythms: https://ecgcourse.com/product/animated-rhythms-course/
helpful
very helpful information however I’m a retired dermatologist
Good illustrations.
Mobitz 1 vs. 2.
It was very helpful. I might like to see a chart format, comparing the characteristics of 2nd degree block types.
We are pleased this was helpful! We do offer the Rhythm Ruler pocket guide card (a laminated clinical tool) that might be helpful. https://ecgcourse.com/product/rhythm-ruler-pocket-guide/