(C) 2024 ECGcourse.com LLC. All rights reserved. | Author: Vernon Stanley MD, PhD | Co-editor: Courtney Stanley, MS, PA-C | Taken from Dr. Stanley’s ECG Courses
In this blog we review the premature beat morphology of 3 different ECG Rhythm premature contractions, namely: PAC (Premature Atrial Contraction), PJC (Premature Junctional Contraction), PVC (Premature Ventricular Contraction).
Please answer the following general 3 questions about premature beats. Answers at bottom of post.
Q1. True or False: The PAC (Premature Atrial Contraction) is readily visible on a rhythm strip and may be seen on any lead of the full 12-lead ECG.
Q2. Based on the intrinsic rate of the AV Node, one would expect a (non-accelerated) junctional rhythm to be:
- A. 20-40 bpm (beats per minute)
- B. 40-60 bpm
- C. 80-100 bpm
- D. Over 100 bpm
Q3. True or False: When a PVC (Premature Ventricular Contraction) occurs in the latter portion of the T-wave during its “vulnerable” period, the “R-on-T Phenomenon” may occur and could trigger Ventricular Tachycardia and sudden death.
Before we begin our discussion of premature beat morphology, let us review some basic terminology. If an area of the heart becomes irritable and discharges early in the cycle, it is called a premature beat. The hallmark of the premature beat is that it occurs earlier in the cycle than expected. The premature beat is named according to its source as follows:
- Premature Atrial Contraction (PAC)
- Premature Junctional Contraction (PJC)
- Premature Ventricular Contraction (PVC)
These are usually benign beats and require no emergency treatment —— one exception might be runs of PVC’s or PVC’s demonstrating the R-on-T phenomena.
Morphology definition according to Webster’s Dictionary: a study of structure or form.
To best analyze the morphology, let us quickly review the propagation of the electrical signal of the ECG Rhythm….
The electrical signal initiates in the SA (Sinoatrial) node, depolarizes the Atrial myocardium, depolarizes the AV node, propagates through the Bundle of HIS, and terminates in the Purkinje cells, depolarizes the Ventricular Myocardium (endocardium to the epicardium). The tissues then recharge (repolarize) and the SA node discharges again, and the cycle repeats itself.
Where:
- 1 = time at depolarization of SA node
- 2 = time at depolarization of AV node
The resultant electrical signal is as follows:
- P = Depolarization of the Atria
- QRS = Depolarization of the Ventricles
- T = Repolarization of the Ventricles
Note: The depolarization of the SA node (at 1) and the AV node (at 2) produce only a tiny voltage and will not be visible on the standard rhythm strip.
3 Morphologies of the Premature Contraction
1. Premature Atrial Contraction (PAC)
Let us return to the PAC (premature atrial contraction) and focus on the regularity or irregularity of the rhythm of the P-P-P pac -P-P intervals. More specifically, I will ask the question: Does a PAC disrupt the regular cadence rhythm of the P-wave?
This question and answer will help recognize or spot PAC’s since they are often a hidden picture, with the Ppac hidden in the QRS or T-wave in the form of a notch or amplification of the QRS-T complex.
There are at least two scenarios to consider:
- First: The PAC discharges at an ectopic focus of the atria and propagates (retrograde) in a wavefront manner to the SA node. This depolarization of the SA node will reset its cadence of automaticity. This will result in a pattern of the P-P-P-P interval of normal-short-long-normal as illustrated on the tutorial.
- Second: The PAC discharges at an ectopic focus of the atria and propagates (retrograde) in a wavefront manner to the SA node. If this wavefront strikes the SA node during it absolute refractory period, the signal will be ignored, and the SA node rhythm cadence will not be disrupted. The P-wave will march thru in a regular manner i.e. P-P-P-Ppac-P-P (all regular except for the Ppac , which will occur early).
2. Premature Junctional Contraction (PJC)
Let us first describe the morphology of a Junctional contraction. If the SA node and the atrial tissues fail to automatically discharge, then the hierarchy of automaticity would expect the AV junction to take command and discharge at its intrinsic rate (40-60 bpm). When this occurs, the resultant is called a junctional rhythm.
As seen in the tutorial below, the atrial myocardium is depolarized in a retrograde direction and consequently you would expect the P-wave to be inverted. This is indeed the case and represents the hallmark of the junctional beat.
We will label this P-wave as: “PJ“
Depending on the propagation time and location of the spontaneous discharge in the AV junction, you will find the following 4 possibilities:
- 1. PJ -wave precedes the QRS complex
- 2. PJ -wave follows the QRS complex
- 3. PJ -wave is buried in the QRS complex
- 4. PJ -wave absent
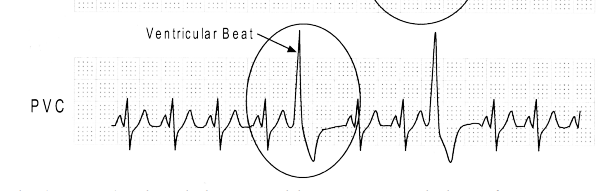
3. Premature Ventricular Contractions
Premature Ventricular Contractions (PVCs) are usually benign beats and most often require no emergency treatment, especially if occurring only as an isolated beat. However, they may reflect underlying heart disease and may require a medical workup.
The morphology of the PVC may vary on the same ECG Rhythm if more than one area of the ventricles becomes irritable and spontaneously discharge, hence designated as multifocal or mulitiform PVCs. This suggests a more irritable ventricle and sometimes will lead to the serious rhythm of Ventricular Tachycardia. This occurrence which may trigger Ventricular Tachycardia, may lead to sudden death and need be noticed and addressed accordingly (with, as always, clinical correlations, labs, clinical presentation, comparison with an old ECG whenever possible and consultation with cardiology and/or hospitalist team.
Patterns of a PVC may be labeled as follows:
- Ventricular Bigeminy: Alternating PVC and normal sinus beat (1:1 ratio)
- Ventricular Trigeminy: 1 PVC followed by 2 normal sinus beats
- Couplets: 2 PVCs in a row
- Ventricular Quadrigeminy: 1 PVC followed by 3 normal sinus beats
- Ventricular Tachycardia: 3 or more PVCs in a row
Now please review this summarization animated tutorial of the Premature Contractions, comparing all 3: PAC, PJC & PVC Morphology
ANSWER Key
Q1. True or False: The PAC (Premature Atrial Contraction) is readily visible on a rhythm strip and may be seen on any lead of the full 12-lead ECG.
Q2. Based on the intrinsic rate of the AV Node, one would expect a (non-accelerated) junctional rhythm to be:
- A. 20-40 bpm (beats per minute)
- B. 40-60 bpm
- C. 80-100 bpm
- D. Over 100 bpm
Q3. True or False: When a PVC (Premature Ventricular Contraction) occurs in the latter portion of the T-wave during its “vulnerable” period, the “R-on-T Phenomenon” may occur and could trigger Ventricular Tachycardia and sudden death.
Enjoy this post? Learn more about our recommended courses:
Animated Rhythms Course (6 hrs Cat I CME)
Compare ALL of Dr Stanley’s ECG and ECG Rhythm Course
Specials & Newsletter SignUp
Form for Specials Page.
2 Responses