(C) 2023 Vernon R Stanley, MD, PhD | Co-editor Courtney Stanley, MS, PA-C | All rights reserved ECGcourse.com, LLC
Please answer the following 3 ECG Interpretation Quiz questions before beginning this case study. Answers will follow at the bottom of this blog post (Questions referenced from Page 14 of the Interactive 12-lead ECG Workbook).
ECG Quiz Question #1: True or False: The requirement |QRS| > or = 0.12 sec is common to both RBBB & LBBB?
A. True
B. False
ECG Quiz Question #2: In a case of RBBB (Right Bundle Branch Block), Lead I is ____ with a broad terminal S-wave.
A. Inverted
B. Upright
C. Flat
D. Biphasic
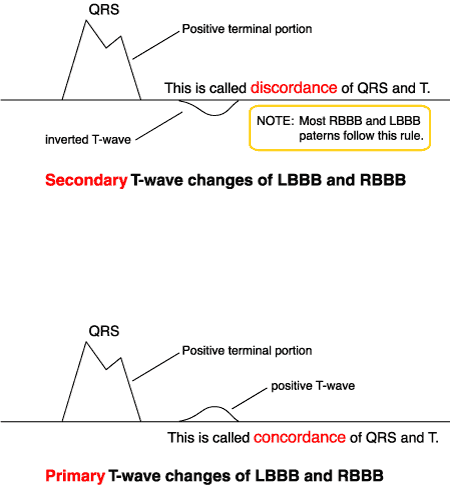
ECG Quiz Question #3: In an otherwise normal case of LBBB & RBBB, if the terminal portion of the QRS complex is positive, the T-wave will be inverted. This is described as ________ T-wave changes.
A. Primary T-wave Changes (or Concordance of the T-waves)
B. Secondary T-wave Changes (or Discordance of the T-waves)
C. Tertiary T-wave Changes (or Accordion Effect of the T-waves)
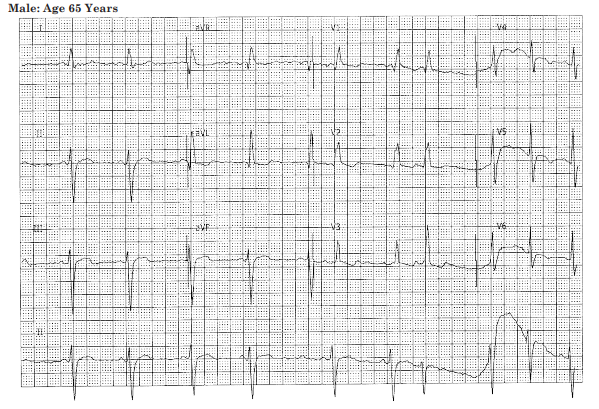
ECG Case Study: We will analyze the following 12-lead ECG of a 65-year-old male who presents with chest pain and is cold, clammy & diaphoretic with an O2 saturation of 97%.
This month’s blog post contains:
- Development of the pattern of The Right Bundle Branch Block (RBBB)
- The focus will be on two ECG Leads: Lead V1 and Lead I
- Primary versus Secondary T-wave Changes
Examining RBBB From Lead V1
- Determine the time of the depolarization wavefront
- Determine the direction of the depolarization wavefront
- Make a judgement of the magnitude of the depolarization wavefront
These three determinations (time, direction, magnitude) will predict the resultant waveform. For Illustrations of the Conduction System of the RBBB (Right Bundle Branch Block | and LBBB):
Diagram #38: The Right Bundle Branch Block (RBBB) Electrical Waves from Lead V1
Please take note of the time sequence of depolarization of the ventricles as follows:
- 1st the Septum is depolarized.
- 2nd the Left Ventricle is depolarized.
- 3rd the Right Ventricle is depolarized.
Next notice the direction of these wavefronts for presentation of Depolarization Wave of Septum and the Left Ventricle
Examining RBBB from ECG Lead I
Now let us develop the waveshape of Lead I associated with the RBBB (Right Bundle Branch Block). Using the same approach as for Lead V1, we will conclude the following: (you are again reminded to concentrate on three aspects of the depolarization wavefronts: direction, timeframe and magnitude, from the perspective of Lead I).
- 1st ……The initial deflection will be downward and rightward ——- Septum
- 2nd …..The next deflection will be downward and leftward ——– Left Ventricle
- 3rd ……The next deflection will be downward and rightward —- Right Ventricle
This resultant ECG waveform from the “viewpoint” Lead I is shown schematically below. (The color coding is the same as for Lead V1.) Remember that the vector representation of Lead I is leftward. Therefore, an electrical signal traveling leftward [the Left Ventricle (colored green) in this situation] will result in a positive deflection on the ECG.
Diagram #41: Predicted Biphasic Waveshape of Lead I in RBBB (Right Bundle Branch Block)
Please observe that this QRS complex has a negative and a positive component, mathematically described as biphasic. Regarding Lead I, our conclusion is as follows: “Lead I is biphasic with a broad terminal S-wave.”
Triad Criteria for the Classic RBBB (Right Bundle Branch Block):
1. QRS Complex Duration = 0.12 sec. (or exceeds)
2. Lead I is biphasic with a broad terminal S-Wave
3. Lead V1 V2 V3 RSR’ (sometimes only small notch, “rabbit ears” or slur)
Primary (Concordance) & Secondary (Discordance) T-wave Changes
If you find an LBBB (Left Bundle Branch Block) or RBBB (Right Bundle Branch Block), you must further analyze all the T-Waves to categorize them as either Primary or Secondary.
If Primary T-Waves are found, this is consistent with ischemia.
- If you find an LBBB, look for Primary and Secondary T’s. (If primary T-wave changes are present, consider myocardial ischemia.)
- If you find an RBBB, look for Primary and Secondary T’s. (Analyze all the Leads looking for ST-Elevation, ST-Depression, T-Wave Peaking and Significant Q’s that might suggest acute ischemia or infarction.)
PEARL: One of the greatest booby traps of electrocardiography is the LBBB. The ST-Elevations, T-wave peaking and significant Q-waves are usually due to the distortion caused by the LBBB conduction i.e. these are usually pseudoinfarction patterns. An exception to this conclusion holds if primary T-waves are present. (When evaluating the Acute Coronary Syndrome (ACS) patient, look for the Modified Sgarbossa Criteria to diagnose the STEMI – aka ST Elevation Myocardial Infarction.)
NOTE: Occasionally you will encounter a cardiogram that demonstrates a widened QRS > 0.10 seconds but otherwise does not meet the classic criteria of the LBBB or RBBB. In order to acknowledge this finding, we label the cardiogram as an IntraVentricular Conduction Delay (IVCD). This is a convenient label to demonstrate that the electrocardiographer recognized the widening of the QRS complex and also that it did not fit the classic criteria pattern of the RBBB or LBBB.
Sometimes it is appropriate to label the tracing as an atypical LBBB or atypical RBBB.
In the above 12-lead ECG, you will notice that 12-lead ECG Leads II, III & avF exhibit very subtle Primary T-wave changes (aka Concordance of the QRS & T–wave). Although soft in presentation on this ECG, this patient was found to have elevated cardiac markers, was diagnosed with an ST Elevation MI (Inferior STEMI) and was sent to the nearest catheterization lab for treatment. As with all cases, it is recommended that in addition to routine labs, serial ECGs, CXR and serial cardiac markers, comparison with an old ECG should be done when possible as well as consultation with the cardiologist. (ECG Case Presentation Referenced from Page 128 of the 12-lead ECG Workbook)
INTERPRETATION of Above Tracing:
- High Voltage Lead avL (probably pseudo due to LAFB – Left Anterior Fascicular Block)
- RBBB (Right Bundle Branch Block) with Primary (Discordance of) T-wave changes
- LAFB (“Left Anterior Fascicular Block” | Bifascicular Block when seen with RBBB)
- ST-elevations (coving) II, III, avF (suspicious of Acute Inferior MI | STEMI)
ECG Quiz Question #1: True or False: The requirement |QRS| > or = 0.12 sec is common to both RBBB & LBBB?
A. True
B. False
ECG Quiz Question #2: In a case of RBBB (Right Bundle Branch Block), Lead I is ____ with a broad terminal S-wave.
A. Inverted
B. Upright
C. Flat
D. Biphasic
ECG Quiz Question #3: In an otherwise normal case of LBBB & RBBB, if the terminal portion of the QRS complex is positive, the T-wave will be inverted. This is described as ________ T-wave changes.
Enjoy this post? View our recommended ECG Course Products


-
Product on sale
 BOGO: 12-lead ECG Course + 50 ECG Case Study Course (43 Hours Cat I CME/CE) | 50% OffOriginal price was: $644.00.$569.00Current price is: $569.00.
BOGO: 12-lead ECG Course + 50 ECG Case Study Course (43 Hours Cat I CME/CE) | 50% OffOriginal price was: $644.00.$569.00Current price is: $569.00. -
Product on sale
 BOGO: 12-lead ECG Course + Animated ECG Rhythm Course (39 Hours Cat I CME/CE)Original price was: $624.00.$559.00Current price is: $559.00.
BOGO: 12-lead ECG Course + Animated ECG Rhythm Course (39 Hours Cat I CME/CE)Original price was: $624.00.$559.00Current price is: $559.00. -
Product on sale
 Unisex HEART Mnemonic Long Sleeve Black T-shirtOriginal price was: $39.50.$34.00Current price is: $34.00.
Unisex HEART Mnemonic Long Sleeve Black T-shirtOriginal price was: $39.50.$34.00Current price is: $34.00. -
Product on sale
 12-lead Textbook, Workbook & HEART Ruler PacketOriginal price was: $124.00.$110.00Current price is: $110.00.
12-lead Textbook, Workbook & HEART Ruler PacketOriginal price was: $124.00.$110.00Current price is: $110.00. -
Product on sale
 50 ECG Case Study & STEMI Review Combo Pack (19 Hrs CME)Original price was: $235.00.$199.00Current price is: $199.00.
50 ECG Case Study & STEMI Review Combo Pack (19 Hrs CME)Original price was: $235.00.$199.00Current price is: $199.00. -
Product on sale
 Starter Online ECG 3-course Suite (22 Hrs CME | ACLS Prep + STEMI + 50 Cases)Original price was: $300.00.$265.00Current price is: $265.00.
Starter Online ECG 3-course Suite (22 Hrs CME | ACLS Prep + STEMI + 50 Cases)Original price was: $300.00.$265.00Current price is: $265.00. -
Product on sale
 Women’s HEART Acronym Fitted T-ShirtOriginal price was: $28.99.$24.00Current price is: $24.00.
Women’s HEART Acronym Fitted T-ShirtOriginal price was: $28.99.$24.00Current price is: $24.00. -
Product on sale
 Cheat Sheet Combo Pack: HEART Mnemonic + ECG Rhythm RulerOriginal price was: $29.00.$18.00Current price is: $18.00.
Cheat Sheet Combo Pack: HEART Mnemonic + ECG Rhythm RulerOriginal price was: $29.00.$18.00Current price is: $18.00. -
Product on sale
 Intensive Triple Bundle ECG Course Suite: (52 Hrs Cat I CME/CE)Original price was: $769.00.$699.00Current price is: $699.00.
Intensive Triple Bundle ECG Course Suite: (52 Hrs Cat I CME/CE)Original price was: $769.00.$699.00Current price is: $699.00. -
Product on sale
 Online ACLS Rhythms Prep Course (3 Hrs CME)Original price was: $65.00.$49.00Current price is: $49.00.
Online ACLS Rhythms Prep Course (3 Hrs CME)Original price was: $65.00.$49.00Current price is: $49.00.
2 Responses